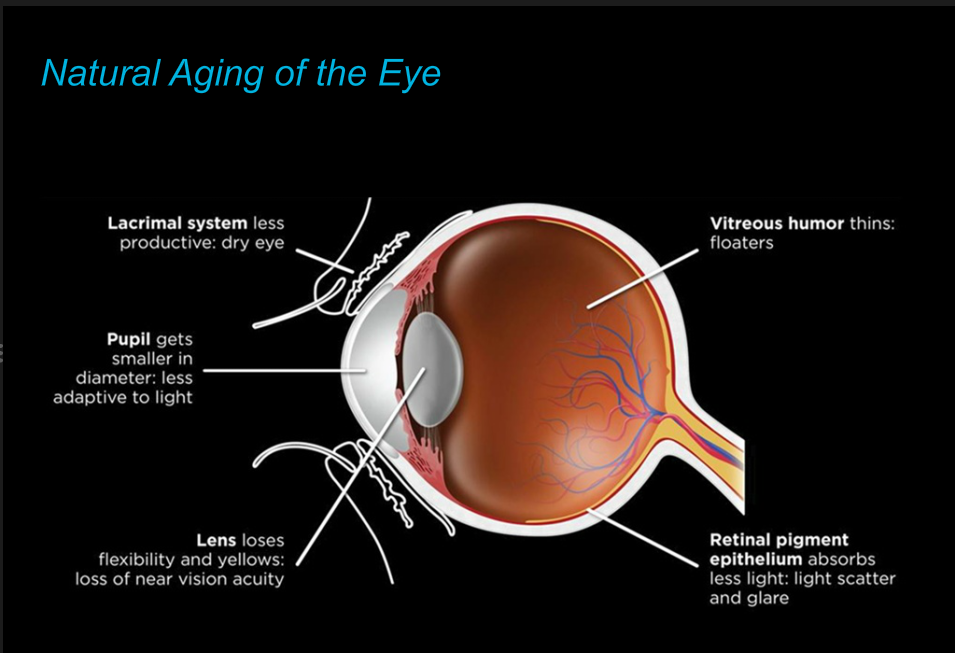
There are a number of changes involving the aging eye which may be of concern to you…
 Here’s a review of some of the common problems middle aged and older patients experience. If you have some of these issues, or simply wish to be evaluated to determine what your visual and eye health status is, call InterMountain Eye Associates for a comprehensive eye exam today. We’re here to serve you and provide the finest eye care in the Pocono Northeast and Northern Tier of Pennsylvania and the Lehigh Valley and southeastern Pennsylvania.
Here’s a review of some of the common problems middle aged and older patients experience. If you have some of these issues, or simply wish to be evaluated to determine what your visual and eye health status is, call InterMountain Eye Associates for a comprehensive eye exam today. We’re here to serve you and provide the finest eye care in the Pocono Northeast and Northern Tier of Pennsylvania and the Lehigh Valley and southeastern Pennsylvania.
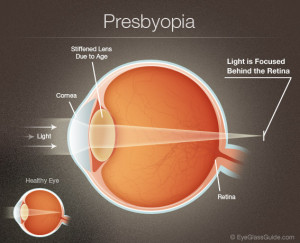
Presbyopia
As we age, human beings undergo many significant changes. One such change that often causes concern for people is the gradual loss of near vision that manifests as we reach our 40’s. This entirely normal process is called presbyopia, literally “old eyes”.
Symptoms of Presbyopia
The symptoms for presbyopia are familiar to anyone over age 45. At first, people notice that after reading for a short time, the words seem to run together. After a brief rest, they can again read for a short time before it happens again. Over time, reading small print – such as numbers in the phone book or the box scores in the newspaper, even items on a menu, becomes harder and often impossible.
People notice that if they hold reading material farther away than normal, the words come into sharper focus. As presbyopia continues to develop, holding reading material farther and farther away is necessary to compensate. Eventually, the arms simply are not longer enough to allow a focal point for clear vision
 Causes of Presbyopia
Causes of Presbyopia
Presbyopia arises due to changes in the lens of the eye. Like a camera lens, the lens of the eye is responsible for adjusting focus.
When we are young, we can easily change focus to look at objects that are nearby or far away. This is because our lenses are young and soft and can quickly and easily change shape to accommodate between distance and near focus, using the muscles of accommodation within the eye. But as we age, the lens becomes stiffer and can no longer easily change shape. As a result, we can no longer adjust our focus to see up close without some help. This most commonly starts around age 43, but can come on a few years earlier in some people, especially in those who are already farsighted.
Treatment for Presbyopia
Help for presbyopia comes in the form of glasses, contacts and more recently, laser vision correction. If you do not use glasses for distance vision then a pair of reading glasses is the easiest solution. Reading glasses are necessary only for up-close tasks such as reading or sewing, and may be removed to see clearly off at a distance. Reading glasses come in different strengths.
Usually weak reading glasses (in the range of +1.25 to +1.50 diopters, or focusing units) will work well when presbyopia symptoms are just beginning, and stronger glasses will be needed every few years until presbyopia stops progressing, usually in your late 60’s. Once presbyopia stops progressing, most people end up with reading glasses in the range of +2.75 to +3.25 diopters.
If you do use glasses for distance vision even before presbyopia starts, a solution for you may involve bifocals or laser vision correction with monovision. Bifocals are glasses that have your distance prescription in the top of the lens and your presbyopic reading prescriptions in the bottom of the lens. The strength of the bifocal part of the lens will have to be increased over the years as presbyopia progresses, just as with reading glasses.
To learn more about Presbyopia link to eyesmart.org.
Glaucoma
An Overview
Glaucoma is a spectrum of eye diseases that share a common feature…the potential to cause blindness by damaging the optic nerve
The eye continuously produces a fluid, called aqueous, which nourishes the internal eye structures such as the lens and the cornea, but that must drain from the eye as well to maintain proper intraocular pressure.
In the most common type of glaucoma, Primary Open Angle Glaucoma, the eye’s drainage canals do not drain efficiently, though they are not visually blocked, and the fluid accumulation cause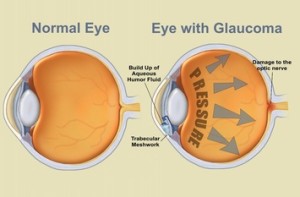 s pressure to build within the eye. This pressure can cause damage to the optic nerve, the conduit for transmitting visual information from the eye to the brain. In other forms of glaucoma, there may be actual mechanical blockage of the drainage structures within the eye, either acutely or on a chronic basis. This is often amenable to laser or surgical correction of the blockage and can sometimes be curative if caught early.
s pressure to build within the eye. This pressure can cause damage to the optic nerve, the conduit for transmitting visual information from the eye to the brain. In other forms of glaucoma, there may be actual mechanical blockage of the drainage structures within the eye, either acutely or on a chronic basis. This is often amenable to laser or surgical correction of the blockage and can sometimes be curative if caught early.
Glaucoma results in peripheral (side) vision loss initially, but the effect is not like looking through a tube or into a tunnel. In fact, most people are not aware of the constriction of their visual field and consequent peripheral vision loss until there has been very extensive damage to the optic nerve. Glaucoma is an especially dangerous eye condition because most people do not experience any symptoms or early warning signs at the onset of glaucoma. This is why glaucoma is often referred to as “the silent thief of sight”.
Glaucoma Can Be Treated, Not Cured
Glaucoma can be treated, but it is not curable. The damage to the optic nerve from glaucoma usually cannot be reversed, except in rare cases when caught early. However, lowering the pressure in the eye often can help to prevent further damage to the optic nerve and loss of peripheral vision. Certain ethnic groups, such as African-Americans and Asians have a much higher incidence of glaucoma than the population as a whole.
Early detection of glaucoma by the staff at InterMountain Eye Associates is the cornerstone of treatment and prevents vision loss and blindness. For most people, treatment for high eye pressure will start with prescription eyedrops. This may include a single drop or a combination of different types, depending on the doctor’s treatment plan and how your body reacts to the medicines. If eyedrops do not lower intraocular pressure enough your doctor may change the drops you’re taking or prescribe laser or conventional glaucoma surgery. Even if you have surgery, it doesn’t necessarily mean you won’t have to take eyedrops in the future, and some types of surgery may need to be repeated. While surgery can lower eye pressure, it cannot restore lost vision.
All of these treatments are meant to preserve the vision you have remaining and help to prevent further loss. Appropriate and ongoing treatment is essential to preserving vision. For those with advanced vision loss due to late diagnosis of glaucoma or from non-compliance with medical therapy, the availability of specialized low vision and vision rehabilitation services can help people with glaucoma live productive and satisfying lives.
Starting as early as age 35 (18 if you are African-American or have a first-order relative with the condition), an eye pressure check for glaucoma should be an essential part of your annual routine eye examination. A visual field test will detect peripheral vision loss and can be performed at the doctor’s discretion. A number of other tests to map the optic nerve, to evaluate it for damage as well as for future comparison, may also be performed to follow the progression of this potentially blinding condition.
Dry Eyes
A dry eye is one of decreased or deficient tears. The medical term for dry eyes is Keratoconjunctivitis Sicca. This deficiency of tears gives rise to inflammation of the eyes. Often there is a burning or gritty feeling and discomfort of the eyes.When present due to the process of aging, it is usually mild but can occasionally be severe and detract from enjoyment of routine activities and life in general.
Paradoxically, there may be episodes of excessive tearing,which is a reflex response to dryness, as well as mucus discharge or blurred vision. In severe cases there can be damage to the cornea and corneal scarring.
This condition can arise from decreased formation of tears, poor quality tears or excessive loss of tears. These can be caused by:
• The natural aging process and menopause
• Disorders seen more frequently in the elderly, such as Rheumatoid Arthritis
• Certain medications
• Eye disorders such as eyelid inflammation
• A dry environment, wind, smoke and air conditioning
Dry eyes should be evaluated by Dr. Vale, a fellowship trained external eye disease and cornea specialist, at InterMountain Eye Associates in Scranton, Carbondale or Bethlehem, PA. The most common treatments for dry eyes are artificial tears drops, gels or ointments. In more severe cases the tears can be retained by using small plugs to block the tear outflow channels. Medical and nutritional therapy for dry eyes is also used when appropriate for the patient. The type of treatment and how often it is used depends on the individual case.
Floaters
Floaters, also known as posterior vitreous separation, is a bothersome condition that can occasionally be a serious problem or can lead to vision loss, particularly when associated with flashing lights (photopsias). The topical was covered in a previous post on this website.
Light Scatter and Poor Illumination That Worsens with Age
The retina is an extension of the brain which lines the back of the eye and is made up of several layers of neurons. It acts like the film in a camera. The back layer of the retina is made up of photoreceptors, special receptor cells that turn light energy into a neural signal. The loss of retinal cells with age, a normal consequence of aging, causes the retina to thin, especially in the periphery. The peripheral retinal cells that survive may exhibit irregular orientations and may direct more toward light entering from the center of the pupil rather than from the peripheral pupil. This change in orientation means that light entering the eye no longer hits the photoreceptors at the same angle as in younger, healthier eyes. This contributes to increased glare in elderly eyes. This is known as the Stiles–Crawford effect.
Reduced retinal illuminance
The retina receives less light as one ages because pupil size becomes smaller (senile miosis) and the crystalline lens becomes thicker and more absorptive. It is estimated that for the same light level, a typical 60-year old receives about one-third the retinal illuminance of a 20-year old.
Reduced contrast and color saturation
The crystalline lens also becomes less clear and, as a result, begins to scatter more light as one ages. Furthermore, the retinal pigment epithelium (RPE), which absorbs stray light rays to reduce glare, doesn’t function as well over age 55 as it does in youth. Additionally, excessive exposure to ultra-violet light by patients who did not make use of UV-blocking sunwear when they were younger can result in degeneration of the RPE with consequent additional light scatter. This scattered light reduces the contrast of the retinal image. This effect also adds a “luminous veil” over colored images on the retina, thus reducing their vividness (saturation). Reds begin to look like pinks, for example.
Reduced ability to discriminate blue colors
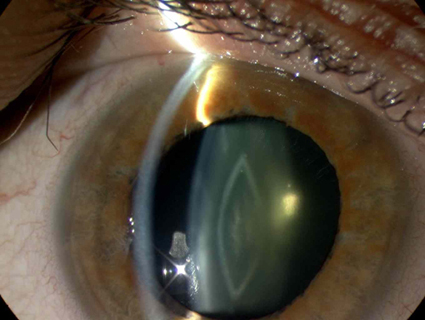
This crystalline lens has become yellow but is not yet a cataract and does not require removal.
The older eye loses some sensitivity to short wavelengths (“blue light”) due to progressive yellowing of the crystalline lens. This can be improved or eliminated through cataract surgery if the lens changes have progressed to the point of a cataract developing. Interestedly, the natural yellowing of the lens with age may be an evolutionary protection developed by the human eye to prevent progressive damage to the retina and other intraocular structures from high energy blue light and even higher energy UV light. In essence, the crystalline lens becomes an internal sunglass!
Help for most age related eye conditions is available at InterMountain Eye Associates, P.C. Call for an appointment. We accept Medicare, Medicare Advantage plans and most major health insurance plans, including high deductible plans and plans associated with medical savings accounts.
Comments are closed